Black men are the least likely group to have access to or receive adequate healthcare in the United States for a variety of reasons. As a result, black men still have some of the worst healthcare outcomes. How can we approach some of these issues to help black men be healthy or become healthcare professionals? UrbanFaith contributor Maina Mwaura interviewed Dr. Jerome Adams, former US Surgeon General and Dr. William Humphries, Neurosurgeon and healthcare expert about Black Men’s health.
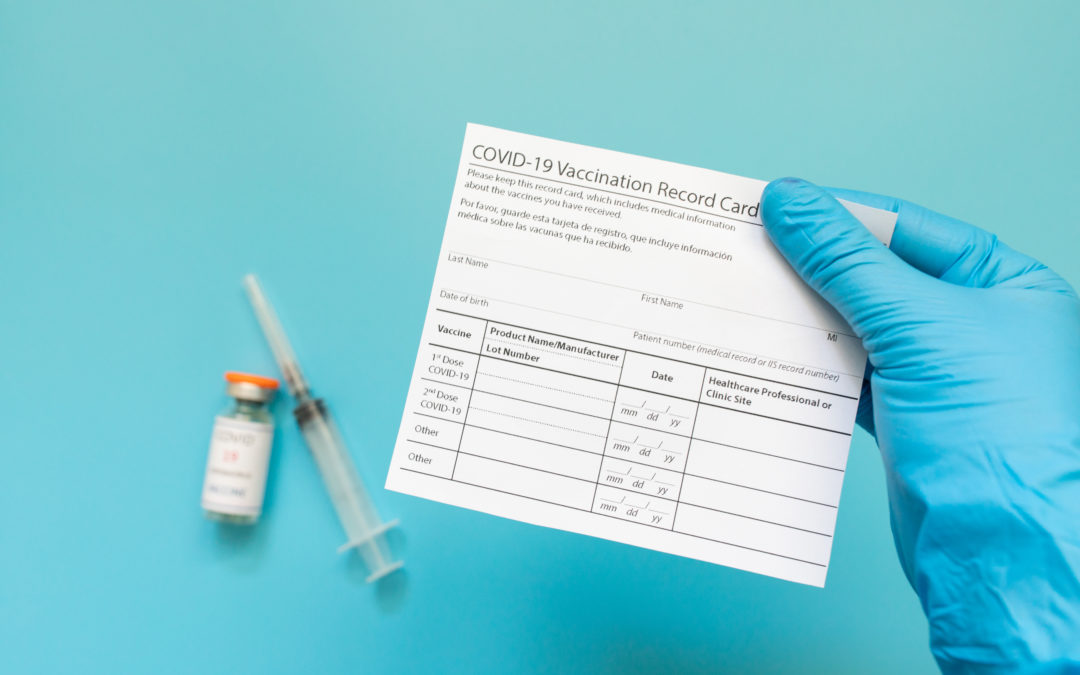
WASHINGTON (RNS) — Earlier this month, the White House announced a “month of action” to help ensure 70% of U.S. adults are at least partially vaccinated by July 4. Officials have since outlined a flurry of faith-based partnerships, hoping to leverage the clout and know-how of faith groups to aid in immunizing the public against COVID-19.
To help explain the role of faith groups in the national vaccine push, Religion News Service spoke with Francis Collins, an evangelical Christian who also serves as director of the National Institutes of Health. Collins discussed the program, as well as his faith and how he views the intersection of religion and science. This interview has been edited for length and clarity.
Why is the government is looking to religious groups for help in vaccination efforts?
It’s nice to be able to have this conversation. As a scientist and a person of faith, this is right in my sweet spot.
People of faith have issues (with vaccines), and every person has some different set they’re concerned about. When getting an answer from a guy like me, a scientist who works for the government, maybe they say, “Well, maybe he has a reason to want us to do this.” But if your pastor says, “I’ve looked at this information and I want what’s best for my congregation. I don’t want to see more people die from this terrible illness that’s taken almost 600,000 American lives. So I’ve educated myself, and I’d like you to know, from me, the benefits and risks. Can we talk about it?” — that gets people’s attention.
While vaccine hesitancy or anti-vaccine sentiment is not unique to any faith group, a recent poll found white evangelicals have a higher-than-average rate of vaccine refusals. But the same poll also found many of them said they could be persuaded by faith-based overtures. Have you seen evidence these overtures are moving the needle?
Yes, although it’s hard to collect really solid data to say how many people changed their minds because they heard from a faith leader. I could give you lots of anecdotes — although the plural of anecdotes is still not data.
I do think it is not a stretch to say, for all of us who’ve prayed for deliverance from COVID-19, the vaccines are an answer to that prayer. That is very much consistent with the way God often responds to our needs — by working through human capabilities that we’ve been given as a gift by the Creator. Why wouldn’t you want to take that gift and not just look at it, but open it up and then roll up your sleeve?
You noted federal government officials aren’t always the most effective messengers to some communities. But as an evangelical Christian, what about your faith compels you to want to embark on this vaccine push?
When you look at what we know about the time Jesus spent on this earth, it is interesting — read through the four Gospels — how many instances where he is involved in healing. If we are called to be followers, as I am, then shouldn’t we also find opportunities to provide healing as well?
If anybody asks you, “Has it been that bad?” Well, gosh, we’ve lost almost 4 million lives on the planet, and almost 600,000 right here in the United States of America. It’s not over, and if we don’t get the vaccinations up to a high enough level, we may see in the fall and the winter a resurgence — particularly in areas where vaccines were least adopted. Then here we are all over again with people in ICUs, people dying that didn’t have to. As believers, is that something we can look away from? I don’t think so.
Many religious communities of color have not only been disproportionately impacted by the pandemic, but also suffer from access issues when it comes to vaccines. Have you seen dividends from efforts by the White House and others to partner with faith groups to help combat those access issues?
Absolutely. That has included some churches that have volunteered to be sites for immunization — right in their fellowship hall. That’s a great thing to do. In this national month of action, we have done additional outreach to those communities that haven’t felt necessarily like they had access, making it possible to get immunized in the barbershop or in the beauty salon, or providing child care for people who might otherwise have trouble figuring out “How am I going to get a shot when I have these two little kids with me that are going to need my attention every second?”
The federal government’s partnership with faith groups in this vaccine push seems unusually robust. What is it about faith communities that makes them particularly beneficial when it comes to vaccination?
As the director of the National Institutes of Health for the last 12 years, we have had partnerships with faith communities for things like hypertension screening, diabetes management and asthma management, but nothing quite like this.
It has been an inspiring occasion, I have to say, to have the opportunity to work side by side with leaders of the faith community to try to get this healing information in front of people. And I hope when we get through COVID-19, which we will, that we won’t lose that.
As a medical expert and a person of faith, what do you think gets left out of disputes between faith groups and the medical community during this pandemic?
One of my goals as a person of faith and a scientist is trying to get people to see the wonderful complementarity and the harmony of scientific and spiritual worldviews.
But I think a lot of people in faith communities haven’t found that to be the case, and maybe have even heard things from the pulpit like “You can’t really trust those scientists because they’re all atheists.” Well, here’s one who’s not, and I’m not alone: About 40% of working scientists are believers in a God who answers prayer. There’s a lot of us out there.
Maybe this is another occasion to try to get a broader understanding about how science and faith are wonderfully complementary. Science is great at answering questions that might start with “how?,” and faith is really good at answering questions that start with “why?” Don’t you, as a person on this planet for a brief glimpse of time, want to be able to ask and maybe get answers to both those types of questions?
Have you seen some of that distrust slip away?
I have, yeah. Going back more than 20 years ago, it did seem like there was a lot of tension for me as an evangelical. There were times where I wasn’t sure I was welcome in the church, and then I’d go to the lab, and I wasn’t sure I was feeling welcomed there either. I wrote a book about this called “The Language of God” back in 2005, trying to put forward arguments about how science and faith really are different ways of looking at God’s creation. It got a lot more attention than I expected.
I think out of that, and a number of other efforts … I do see there has been a shift here, more of a willingness to consider what the harmony is instead of what the battle is.
Are you optimistic the U.S., with the help of faith communities, can meet this July Fourth deadline to partially vaccinate 70% of the adult population?
I am optimistic, but it’s going to be a stretch. It’s going to take the full efforts of lots and lots of people — and especially faith communities — to get us there over what is just another three weeks.
The number of immunizations happening each day is just barely on that pathway, and it actually looks as if some of those immunization levels are dropping instead of going up. We need everybody to line up behind this goal, recognizing this isn’t about pleasing Joe Biden, because a lot of evangelicals are not that interested in pleasing Joe Biden. This is about saving lives.
Could your medical treatment one day be tailored to your DNA? That’s the promise of “personalized medicine,” an individualized approach that has caught the imagination of doctors and researchers over the past few years. This concept is based on the idea that small genetic differences between one person and another can be used to design tailored treatments for conditions as diverse as cancer and schizophrenia.
In principle, “personalized” is not meant to mean one person but not another, though that may not turn out to be the case. Existing genetic and medical research data conspicuously underrepresent certain populations.
Case in point: Last month, researchers published a surprising study on youth suicide rates. Scientists long believed that white youth had the highest rates of suicide. But, examining data from the Centers for Disease Control and Prevention, they found that suicide rates for African-American children under the age of 13 were twice as high as whites.
This finding turned long-held assumptions about racial imbalances in mental illness on its head. It could not be explained by economic circumstances, suggesting that there are other factors at play, perhaps even genetic factors. Suicide is a complicated personal act, but science has shown that genes play an important role.
This unexpected result may have implications for prevention and treatment based on genes – in other words, personalized medicine. But the state of current genetic research suggests that African-Americans will likely miss out on many of the potential future benefits of personalized medicine.
As lead author Jeffrey Bridge of the Nationwide Children’s Hospital in Ohio noted to the Washington Post, “Most of the previous research has largely concerned white suicide. So, we don’t even know if the same risk and protective factors apply to black youth.”
Few experts have studied the possible genetic causes for African-American suicide, focusing instead on environmental and social reasons.
While most mental illnesses such as depression are first diagnosed in adulthood, they actually have their origins early in development, as genes and the environment interact to shape the brain of a growing fetus. For example, my colleagues and I published a study in May showing that genes and pregnancy problems combine to increase the likelihood of schizophrenia.
This should cause some alarm, because African-American women have much higher rates of pregnancy complications. Black infants die at twice the rate of white infants. Again, this is not explained by socioeconomic reasons.
In short, a higher rate of pregnancy problems likely puts African-Americans at increased risk of developing mental illnesses, perhaps explaining the noticeable increased rate of suicides. Additional genetic data on this population could potentially illuminate the issue.
To better understand genes that increase the risk for mental illness, researchers study the brains of people who have died. They examine how genetic differences could have led to changes in the brains of people who developed these conditions. This is one of the best ways to understand any brain disorder at a biological level.
But African-Americans are underrepresented in large-scale genetic and neuroscience studies. One 2009 analysis revealed that 96 percent of participants in large genetic studies were of European descent. When researchers looked at the matter a couple of years ago, they found that the proportion of people with African ancestry in these studies had increased by only 2.5 percent. Similarly, studies of African-American brains are almost nonexistent.
Why the low participation rate? One reason is that researchers favor populations that are genetically more homogeneous to ensure a study’s accuracy. Individuals of European ancestry are more alike genetically than are African-Americans.
Some experts have posited that African-Americans are less likely to participate in genetic studies due to a lack of trust with the medical community.
At the Lieber Institute for Brain Development, where I work, people can donate the brains of family members who wished to contribute to scientific research. We have the largest collection of African-American brains donated to study mental illness, though it’s relatively small in comparison to the availability of Caucasian brains. In our experience, the donation rate for African-American families is comparable to that of white families, suggesting that lack of trust may not be as widespread as believed.
Without studies focused on the African-American brain, scientists will struggle to fully understand how any possible unique genetic risk in the African-American population translates into prevention and treatment for virtually all disorders that involve the brain, including suicide.
Researchers have to invest in correcting this shortcoming before the personalized medicine train is so far out of the station that the African-American community cannot get on it.
Daniel R. Weinberger, Director of the Lieber Institute for Brain Development and Professor, Departments of Psychiatry, Neurology, Neuroscience and The Institute of Genetic Medicine, Johns Hopkins University