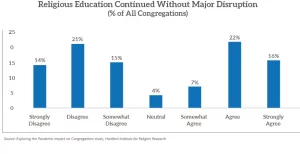
(RNS) — Sunday school and other Christian education programs have suffered during the COVID-19 pandemic, with half of congregations surveyed saying their programs were disrupted.
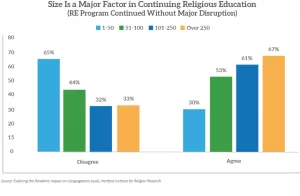
A March 2022 survey by the Hartford Institute for Religion Research found that larger churches with more than 100 people were more successful in maintaining their educational programming for children and youth, often using in-person or hybrid options. Smaller churches, especially those with 50 or fewer attendees, were least likely to say they continued religious education without disruption.
Scott Thumma, principal investigator of the Exploring the Pandemic Impact on Congregations project, said the findings echoed concerns about general education of schoolchildren, where researchers have seen declines in learning over the last two years.
“My sense is that people knew what good robust Sunday school was or what a successful vacation Bible school was,” said Thumma, drawing in part on open-ended comments in the survey. “And they couldn’t parallel that using Zoom or using livestreaming or using take-home boxes of activities. It just wasn’t the same thing. And so when they evaluated it, it just didn’t measure up to what they previously knew as the standard of a good quality religious education program.”
The findings are the third installment in the five-year project, a collaboration with 13 denominations from the Faith Communities Today cooperative partnership and institute staffers.
The new report, “Religious Education During the Pandemic: A Tale of Challenge and Creativity,” is based on responses from 615 congregations across 31 denominations.
Comparing data from 2019, churches surveyed in March 2022 reported that the attendance of their religious education programs had decreased an average of 30% among children younger than 13 and 40% among youth, ages 13-17.
“Analysis showed that those who closed their programs had the greatest decline in involvement even after they restarted,” the new report states. “Likewise, churches that moved religious education online lost a higher percentage of participants than churches who modified their efforts with safety protocols but continued meeting in person either outdoors or in small groups.”
The report notes that it’s not surprising the smallest churches experienced the most disruption in their religious education, given the decline in volunteer numbers and additional stresses on clergy during the pandemic.
“In the smallest churches (1-50 attendees) pastors were most likely in charge of the religious education programs, while for those between 51 and 100 worshippers, volunteers bore the bulk of leadership responsibilities,” according to the report.
Overall, evangelical churches reported experiencing the least disruption to their educational programs, while mainline churches reported the most, followed by Catholic and Orthodox congregations.
Vacation Bible school, long a staple of congregational outreach to local communities, has also been shaken by COVID-19. More than a third (36%) of churches offered such programs prior to the pandemic. That number decreased to 17% in 2020 and jumped back to 36% in the summer of 2021. Slightly less than a third (31%) reported VBS plans for 2022.
While children’s programming was greatly affected by congregational change during the pandemic, adult religious programs saw the smallest decreases compared with pre-pandemic levels, with a quarter growing since 2019 and an almost equal percentage (23%) remaining even.
But, as with children’s programs, churches with 50 or fewer worshippers saw the greatest loss in adult religious education, while those with more than 250 in worship attendance increased their adult programs by an average of 19%.
Some congregations reported moving Sunday school activities to weeknights or vacation Bible schools from weekday mornings to later hours, with mixed results.
“One said they ‘went from a typical 200+ kids to about 35,’” the report notes, and they “’shortened the number of days and moved VBS to the afternoon.’”
Thumma said innovations including intergenerational and kid-friendly programming helped sustain programs for people of all ages in some congregations. These included revamping of the children’s message time during worship to be more inclusive or older members greeting children who run by during Zoom sessions. Some churches called their all-ages activities “messy church” or “Sunday Funday” as they used interactive educational events.
“It becomes, out of necessity, intergenerational because that allows you to have robust energy and lots of people there,” he said. “But it really is directed at the kids being involved in the life of the congregation in a way that isn’t, like, ‘OK, you go to your class’ and ‘you go to your classes,’ and the classes don’t ever mingle.”
Whether creative steps such as new intergenerational activity will continue remains to be seen, Thumma added.
“I think it should because that’s a valuable strategy,” he said. “One of the things that we’ve seen in lots of our research is the more intergenerational the congregation is, the more it has a diversity of any degree, the more likely they are to be vital and thriving.”
The findings in the new report of the project, which is funded by the Lilly Endowment, have an estimated overall margin of error of plus or minus 4 percentage points.
(RNS) — The devastating COVID-19 health crisis has become an economic crisis for millions of people — but not for everyone. Last year, families across the United States struggled to put food on the table and balance the responsibilities of childcare and work (assuming they still had a job), but the wealthiest people in our country only got wealthier.
That wealth has not trickled down to families who are struggling to pay their rent, feed their children and create an economically secure quality of life.
The American Rescue Plan — the COVID-19 relief bill passed in March — expanded eligibility for two of the most vital anti-poverty programs we have. It made the Child Tax Credit fully refundable, fixing the gap that excluded families in poverty from receiving the same benefits as their higher-earning counterparts.
It also expanded the Earned Income Tax Credit for workers without children, young workers ages 19-24 and older workers over age 65.
Both adjustments put more money into the pockets of low-income people who were previously ineligible — many of them frontline workers in the pandemic. But these payments will expire on Dec. 31 if Congress does not extend them.
These tax credits work, and, not surprisingly, they are wildly popular. The Child Tax Credit provides a lifeline of economic support to families nationwide who need money to pay for daycare, groceries, utilities, rent, and health care bills that pile up nonstop. This is money being pumped back into local economies coast to coast right now, creating a virtuous economic cycle of helping people in need and local business.
Recently, I spoke with Barbie Izquierdo on the value of programs like these. An advocate and consultant who eloquently gives voice for food justice based on her personal experience, Barbie told me that despite all her work — sometimes full time, sometimes part time, often working more than one job — she “would still come home to an empty fridge.” Her story is shared by hundreds of thousands of families across our country.
To this day, the tax credits are one of the primary barriers keeping Barbie from falling back into poverty as she raises her 14- and 16-year-old children as a single mother. “(They) help you catch up and it alleviates some of the burden of being reminded that you’re poor. They’ve definitely helped me on many occasions,” she explained. “Who knows if I would be here today if I didn’t have that help?”
Since July, millions of families have been receiving Child Tax Credit checks each month. The latest government data indicates that these robust federal programs have put a dent in poverty, which has cascading benefits for children now and in their future — if we can keep these programs in place past the end of the year.
As Congress continues to negotiate additional recovery legislation, we have a historic opportunity to permanently invest in the future of our children. Congress should seize this moment to not only give immediate help to tens of thousands of their constituents but also to strengthen our country’s future.
Specifically, we must adjust the tax code that bends over backward for the extremely wealthy while treating those who struggle every day to afford food and housing as a burden. The more Congress can raise in revenue, the bigger the opportunity we have to address poverty and hunger while investing in our children. It takes real political will to require corporations and the wealthiest among us to pay their fair share. But we expect nothing less.
As a Quaker, my faith and practice encourage me to treat every person as a beloved child of God, which means I am called to do all I can to foster a more equitable, ethical world in which every person can flourish.
I believe Congress wants to help families in need, to ensure a better world for all. This is their opportunity to support the full refundability of the Child Tax Credit. This is the political moment when we can make transformational change in our country.
( Diane Randallis the general secretary of the Friends Committee on National Legislation, a national, nonpartisan Quaker lobby for peace, justice, and the environment. The views expressed in this commentary do not necessarily reflect those of Religion News Service.)
During the COVID-19 pandemic many people faced homelessness, hunger, and loss as a result of the coronavirus and related shut-downs. But one newly opened restaurant outside Sacramento, California was able not only to survive the pandemic, but thrive and help others survive in the midst of it.
UrbanFaith sat down with Chef Q who is the Executive Chef & Owner of Q1227 restaurant outside of Sacramento as he shared his recipe not only to survive, but thrive as an restauranteur, person of faith, and community catalyst in the midst of the pandemic. His restaurant was able to feed over 40,000 homeless and in need families in 2020 and he has made his restaurant one of the most impactful and successful institutions in his community. The full interview is above.
This story is from a partnership that includes NPR, KQED and KHN.
For months, journalists, politicians and health officials — including New York Gov. Andrew Cuomo and Dr. Anthony Fauci — have invoked the infamous Tuskegee syphilis study to explain why Black Americans are more hesitant than white Americans to get the coronavirus vaccine.
“It’s ‘Oh, Tuskegee, Tuskegee, Tuskegee,’ and it’s mentioned every single time,” said Karen Lincoln, a professor of social work at the University of Southern California and founder of Advocates for African American Elders. “We make these assumptions that it’s Tuskegee. We don’t ask people.”
When she asks Black seniors in Los Angeles about the vaccine, Tuskegee rarely comes up. People in the community talk about contemporary racism and barriers to health care, she said, while it seems to be mainly academics and officials who are preoccupied with the history of Tuskegee.
“It’s a scapegoat,” Lincoln said. “It’s an excuse. If you continue to use it as a way of explaining why many African Americans are hesitant, it almost absolves you of having to learn more, do more, involve other people — admit that racism is actually a thing today.”
It’s the health inequities of today that Maxine Toler, 72, hears about when she asks her friends and neighbors in Los Angeles what they think about the vaccine. As president of her city’s senior advocacy council and her neighborhood block club, Toler said she and most of the other Black seniors she talks with want the vaccine but are having trouble getting it. And that alone sows mistrust, she said.
Toler said the Black people she knows who don’t want the vaccine have very modern reasons for not wanting it. They talk about religious beliefs, safety concerns or a distrust of former U.S. President Donald Trump and his contentious relationship with science. Only a handful mention Tuskegee, she said, and when they do, they’re fuzzy on the details of what happened during the 40-year study.
“If you ask them ‘What was it about?’ and ‘Why do you feel like it would impact your receiving the vaccine?’ they can’t even tell you,” she said.
Toler knows the details, but she said that history is a distraction from today’s effort to get people vaccinated against the coronavirus.
“It’s almost the opposite of Tuskegee,” she said. “Because they were being denied treatment. And this is like, we’re pushing people forward: Go and get this vaccine. We want everybody to be protected from covid.”
Questioning the Modern Uses of the Tuskegee Legacy
The “Tuskegee Study of Untreated Syphilis in the Negro Male” was a government-sponsored, taxpayer-funded study that began in 1932. Some people believe that researchers injected the men with syphilis, but that’s not true. Rather, the scientists recruited 399 Black men from Alabama who already had the disease.
Researchers told the men they had come to Tuskegee to cure “bad blood,” but never told them they had syphilis. And, the government doctors never intended to cure the men. Even when an effective treatment for syphilis — penicillin — became widely available in the 1940s, the researchers withheld it from the infected men and continued the study for decades, determined to track the disease to its endpoint: autopsy.
By the time the study was exposed and shut down in 1972, 128 of the men involved had died from syphilis or related complications, and 40 of their wives and 19 children had become infected.
Given this horrific history, many scientists assumed Black people would want nothing to do with the medical establishment again, particularly clinical research. Over the next three decades, various books, articles and films repeated this assumption until it became gospel.
“That was a false assumption,” said Dr. Rueben Warren, director of the National Center for Bioethics in Research and Health Care at Tuskegee University in Alabama, and former associate director of minority health at the Centers for Disease Control and Prevention from 1988 to 1997.
A few researchers began to question this assumption at a 1994 bioethics conference, where almost all the speakers seemed to accept it as a given. The doubters asked, what kind of scientific evidence is there to support the notion that Black people would refuse to participate in research because of Tuskegee?
When those researchers did a comprehensive search of the existing literature, they found nothing.
“It was apparently a ‘fact’ known more in the gut than in the head,” wrote lead doubter Dr. Ralph Katz, an epidemiologist at the New York University College of Dentistry.
So Katz formed a research team to look for this evidence. They completed a series of studies over the next 14 years, focused mainly on surveying thousands of people across seven cities, from Baltimore to San Antonio to Tuskegee.
The conclusions were definitive: While Black people were twice as “wary” of participating in research, compared with white people, they were equally willing to participate when asked. And there was no association between knowledge of Tuskegee and willingness to participate.
“The hesitancy is there, but the refusal is not. And that’s an important difference,” said Warren, who later joined Katz in editing a book about the research. “Hesitant, yes. But not refusal.”
Tuskegee was not the deal breaker everyone thought it was.
These results did not go over well within academic and government research circles, Warren said, as they “indicted and contradicted” the common belief that low minority enrollment in research was the result of Tuskegee.
“That was the excuse that they used,” Warren said. “If I don’t want to go to the extra energy, resources to include the population, I can simply say they were not interested. They refused.”
If you say Tuskegee, then you don’t have to acknowledge things like pharmacy deserts, things like poverty and unemployment,
Karen Lincoln
Now researchers had to confront the shortcomings of their own recruitment methods. Many of them never invited Black people to participate in their studies in the first place. When they did, they often did not try very hard. For example, two studies of cardiovascular disease offered enrollment to more than 2,000 white people, compared with no more than 30 people from minority groups.
“We have a tendency to use Tuskegee as a scapegoat, for us, as researchers, not doing what we need to do to ensure that people are well educated about the benefits of participating in a clinical trial,” said B. Lee Green, vice president of diversity at Moffitt Cancer Center in Florida, who worked on the early research debunking the assumptions about Tuskegee’s legacy.
“There may be individuals in the community who absolutely remember Tuskegee, and we should not discount that,” he said. But hesitancy “is more related to individuals’ lived experiences, what people live each and every day.”
‘It’s What Happened to Me Yesterday’
Some of the same presumptions that were made about clinical research are resurfacing today around the coronavirus vaccine. A lot of hesitancy is being confused for refusal, Warren said. And so many of the entrenched structural barriers that limit access to the vaccine in Black communities are not sufficiently addressed.
Tuskegee is once again being used as a scapegoat, said Lincoln, the USC sociologist.
“If you say ‘Tuskegee,’ then you don’t have to acknowledge things like pharmacy deserts, things like poverty and unemployment,” she said. “You can just say, ‘That happened then … and there’s nothing we can do about it.’”
She said the contemporary failures of the health care system are more pressing and causing more mistrust than the events of the past.
“It’s what happened to me yesterday,” she said. “Not what happened in the ’50s or ’60s, when Tuskegee was actually active.”
The seniors she works with complain to her all the time about doctors dismissing their concerns or talking down to them, and nurses answering the hospital call buttons for their white roommates more often than for them.
As a prime example of the unequal treatment Black people receive, they point to the recent Facebook Live video of Dr. Susan Moore. When Moore, a geriatrician and family medicine physician from Indiana, got covid-19, she filmed herself from her hospital bed, an oxygen tube in her nose. She told the camera that she had to beg her physician to continue her course of remdesivir, the drug that speeds recovery from the disease.
“He said, ‘Ah, you don’t need it. You’re not even short of breath.’ I said ‘Yes, I am,’” Moore said into the camera. “I put forward and I maintain, if I was white, I wouldn’t have to go through that.”
Moore died two weeks later.
“She knew what kind of treatment she should be getting and she wasn’t getting it,” said Toler of L.A., contrasting Moore’s treatment with the care Trump received.
“We saw it up close and personal with the president, that he got the best of everything. They cured him in a couple of days, and our people are dying like flies.”
Toler and her neighbors said that the same inequity is playing out with the vaccine. Three months into the vaccine rollout, Black people made up about 3% of Californians who had received the vaccination, even though they account for 6.2% of the state’s covid deaths.
The first mass-vaccination sites set up in the Los Angeles area — at Dodger Stadium and at Disneyland — are difficult to get to from Black neighborhoods without a car. And you practically needed a computer science degree to get an early dose, as snagging an online appointment required navigating a confusing interface or constantly refreshing the portal.
It’s stories like these, of unequal treatment and barriers to care, that stoke mistrust, Lincoln said. “And the word travels fast when people have negative experiences. They share it.”
To address this mistrust will require a paradigm shift, said Warren of Tuskegee University. If you want Black people to trust doctors and trust the vaccine, don’t blame them for their distrust, he said. The obligation is on health institutions to first show they are trustworthy: to listen, take responsibility, show accountability and stop making excuses. That, he added, means providing information about the vaccine without being paternalistic and making the vaccine easy to access in Black communities.
“Prove yourself trustworthy and trust will follow,” he said.
This story is from a partnership that includes NPR, KQED and KHN.
For the past 15 years my family tradition is to travel from Washington, D.C., along with both grandparents, to sunny Florida to celebrate Thanksgiving with cousins. This year we decided to skip the travel and will have fall and winter celebrations at home.
We are not canceling the holidays, but to keep ourselves and others safe, we are keeping plans small and flexible and remembering that the health of those we love is most important as we enter the season of gratitude.
Maintaining vigilant social distancing, mask-wearing and good hygiene in the weeks leading up to the holidays are the first steps to reduce risk. AP Photo/Rich Pedroncelli
Before you gather
First, it is important that everyone who will be attending any holiday celebration is on the same page about how to take precautions before getting together. The idea is to lower infection risk in the weeks leading up to the holidays and then test to confirm.
In conjunction with quarantining, testing is the second strategy.
Research has consistently shown that people are most contagious a day or two before they show symptoms, so everyone plans to get tested with an RT-PCR test within 72 hours of Thanksgiving, while still being able to get results in hand before we gather.
If the demand for tests is high and wait times are long, we will get rapid tests. But these are a second choice, as they are less reliable and can be expensive.
Where and how to eat and socialize
No matter how careful you and your family are, there is some risk that someone will be infected. With that in mind, the goal is to reduce the conditions that lead to viral spread. The biggest risks are indoor spaces with poor ventilation, large groups and close contact. So we are planning the opposite: a short outdoor Thanksgiving with a small group and plenty of space between everyone.
To reduce the risk of infection from flying and to keep the gathering small, the only people coming to Thanksgiving at my family’s home in D.C. are my mother, my aunt and my uncle – all of whom live within driving distance. This is in addition to myself, my husband and our kids. When deciding how many people will come to the holidays, keep it small and consider the amount of space you have to maintain social distancing.
If the weather cooperates, we plan to be outside for trivia games and the turkey meal. Rather than eat around one table, we will have individual tables and place settings spaced far apart and space heaters around. I’ve got a mini care package planned for each guest so that everyone will have their own blanket, hand sanitizer, utensils and a festive mask. My mother won’t be helping out in the kitchen this year and, unfortunately, that goes for cleanup too. We won’t take a group picture but I will be sure to capture some of the special moments.
If the weather doesn’t cooperate, Plan B is to be inside in the large family room with as many windows open as possible and with everyone spaced as far apart as possible. Being outside is safer, but if you must be indoors, improve ventilation by opening doors and windows. Consider turning on exhaust fans and using an air purifier.
Everyone who lives in the household will be in one section while my mom will have her own individual area, as will my aunt and uncle. Even though we won’t hold hands before sharing the meal, we will still recite that we are “thankful for family, friends and food.”
Whether outside or inside, everyone will wear masks when they aren’t eating, maintain 6 feet of distance and use the hand sanitizer that I will place throughout the house.
It is also important to be mindful of alcohol consumption, as a pandemic is not the time for lowered inhibitions and bad judgment.
After the event
I hope everyone enjoys the meal and quality time spent with one another in this melancholy year, but the work is not done once the dishes are clean and everyone is home safely.
Everyone is planning to get another COVID–19 test one week after the meal. Additionally, Thanksgiving is our family’s trial run for Christmas, so a few days after, I plan to call everyone and discuss what worked well and what didn’t. If all goes well, I hope to repeat this quarantine, test and gather process for Christmas.
The ending of 2020 deserves to be celebrated, given this difficult year. This Thanksgiving will be different from those of other years, and my kids understand they need to manage their expectations. But we still plan to uphold our tradition of writing all that we are thankful for and reading our messages aloud to one another. We will still share love, some laughs and a good meal while everyone does their part to protect one another.