NASHVILLE, Tenn. — Just before students at Meharry Medical College went home for Thanksgiving, Dr. James Hildreth, the school’s president, emailed them a video message that he acknowledged seemed hard to believe. Or at least they had to give it a second listen.
“We’ll gift each of you $10,000 in cash,” he said, looking at the camera. “You heard me right.”
They were told to expect a direct deposit the next day or pick up a check in person. Hildreth, an expert in infectious diseases who helped lead Nashville’s pandemic response, explained that this gift with no strings attached was money from the CARES Act, a major covid-19 relief law passed by Congress in 2020. He asked only that they be “good stewards” of the windfall.
After deep consideration, Meharry’s administration decided to give roughly a third of its CARES Act funding — $10 million — directly to its future doctors, dentists and public health researchers. All told, 956 students received payments.
Meharry’s students had already been heavily involved in the pandemic response, staffing Nashville’s mass covid testing and vaccination sites. But the money isn’t so much surprise compensation for volunteer efforts as it is an investment in a future career — and an assist in overcoming financial hurdles Black students especially face to become medical professionals.
While Black Americans make up roughly 13% of the population, the Association of American Medical Colleges finds Black doctors account for just 5% of the nation’s working physicians — a figure that has grown slowly over more than a century. And studies have found that Black patients often want to be cared for by someone whom they consider culturally competent in acknowledging their heritage, beliefs and values during treatment.
“We felt that there was no better way to begin distributing these funds than by giving to our students who will soon give so much to our world,” Hildreth said.
Cheers erupted in the library as students clicked the video link.
Andreas Nelson fell silent, he recalled later. He went to his banking app and stared in disbelief. “$10,000 was sitting just in my bank account. It was astonishing,” he said. “I was literally lost for words.”
The Chicago native is finishing a master’s degree in health and science at Meharry with hopes of entering its dental school. The average student loan debt in the programtotals more than $280,000. So, undoubtedly, 10 grand won’t make much of a dent in the debt.
But the money in his pocket eases his top concern of making rent each month. Nelson said it feels as though he’s being treated like an adult, allowing him to decide what his greatest needs are in getting through school.
“It’s motivating,” Nelson said. “Because that means they have trust in us to do with this money whatever the cause may be — whether it be student debt, investing or just personal enjoyment.”
Across the board, students at HBCUs rely more on student loans than students at historically white institutions. Roughly 80% take out student loans, according to an analysis by UNCF, formerly known as the United Negro College Fund, and they borrow considerably more.
Meharry was founded a decade after the Civil War to help those who had been enslaved. But the 145-year-old institution has always struggled financially, and so have its students.
Meharry’s average student debt is far higher than other area schools of medicine at Vanderbilt University and the University of Tennessee, representing both private and public institutions.
Virtually all colleges and universities received allotments under the CARES Act, but HBCUs have been much more aggressive about funneling substantial amounts directly to students, who tend to have greater need. More than 20 HBCUs have erased outstanding tuition balances. Some have canceled student fees.
But Meharry, one of the few stand-alone HBCU graduate schools, is a rare case in cutting checks for students.
“These young people are rising to medical school against all odds,” said Lodriguez Murray, who leads public policy and government affairs at UNCF. “Of course, they have to borrow more because people who look like them have less.”
During the pandemic, major philanthropists have taken new interest in supporting the few HBCU medical schools. Michael Bloomberg committed $100 million to four institutions, including Meharry, to help educate more Black doctors.
Students at Meharry can now apply for $100,000 scholarships. The $34 million from Bloomberg Philanthropies is also going toward other kinds of financial support.
The school is now offering, for no additional fee, expensive test-prep services through a Boston-based company, MedSchoolCoach. The service, which entails paying a doctor by the hour to help with studying, can cost thousands of dollars.
While the price is often out of reach for students tight on cash, acing the benchmark exams toward board licensure is key to landing coveted fellowships, qualifying for lucrative specialties or just finishing on time. And Meharry’s four-year completion rate of roughly 70% is below most schools. The most up-to-date national average is around 82%.
For some, Murray said, a $10,000 windfall may make all the difference in whether they cross the finish line and become a doctor who can afford all their medical school debt.
“Many of those students are borrowing a lot of money to complete their dream, and to become relatively high earners in the future,” Murray said. “The fact that these students are largely coming from lower socioeconomic backgrounds means that the funds that Meharry turned around and gave to the students are particularly impactful.”
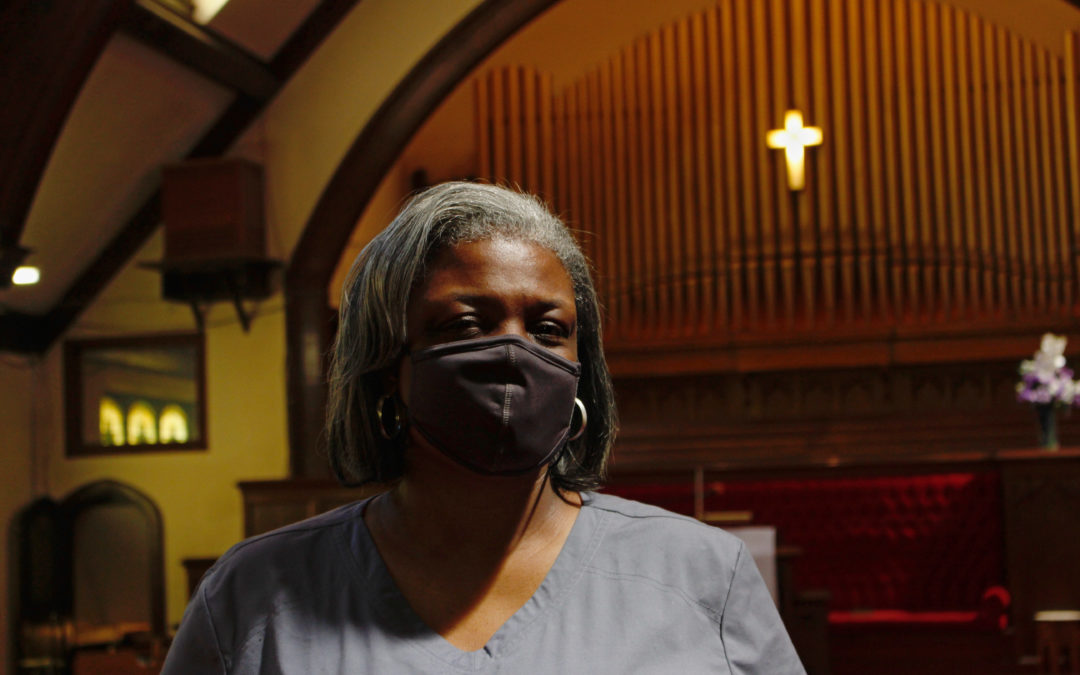
In this May 9, 2021, photo, Rev. Joseph Jackson Jr. talks to his congregation at Friendship Missionary Baptist Church in Milwaukee during a service. He is president of the board of directors for Milwaukee Inner City Congregations Allied for Hope, which along with Pastors United, Souls to the Polls and the local health clinic Health Connections, is working to get vaccination clinics into churches to help vaccinate the Black community. He’s also been urging his congregation during Sunday services to get vaccinated. (AP Photo/Carrie Antlfinger)
MILWAUKEE (AP) — Every Sunday at Friendship Missionary Baptist Church, the Rev. Joseph Jackson Jr. praises the Lord before his congregation. But since last fall he’s been praising something else his Black community needs: the COVID-19 vaccine.
“We want to continue to encourage our people to get out, get your shots. I got both of mine,” Jackson said to applause at the church in Milwaukee on a recent Sunday.
Members of Black communities across the U.S. have disproportionately fallen sick or died from the virus, so some church leaders are using their influence and trusted reputations to fight back by preaching from the pulpit, phoning people to encourage vaccinations, and hosting testing clinics and vaccination events in church buildings.
Some want to extend their efforts beyond the fight against COVID-19 and give their flocks a place to seek health care for other ailments at a place they trust — the church.
In this May 9, 2021, photo, Rev. Joseph Jackson Jr. talks to his congregation at Friendship Missionary Baptist Church in Milwaukee during a service. He is president of the board of directors for Milwaukee Inner City Congregations Allied for Hope, which along with Pastors United, Souls to the Polls and the local health clinic Health Connections is working to get vaccination clinics into churches to help vaccinate the Black community. He’s also been urging his congregation during Sunday services to get vaccinated. (AP Photo/Carrie Antlfinger)
“We can’t go back to normal because we died in our normal,” Debra Fraser-Howze, the founder of Choose Healthy Life, told The Associated Press. “We have health disparities that were so serious that one pandemic virtually wiped us out more than anybody else. We can’t allow for that to happen again.”
Choose Healthy Life, a national initiative involving Black clergy, United Way of New York City and others, has been awarded a $9.9 million U.S. Department of Health and Human Services grant to expand vaccinations and and make permanent the “health navigators” who are already doing coronavirus testing and vaccinations in churches.
The navigators will eventually bring in experts for vaccinations, such as the flu, and to screen for ailments that are common in Black communities, including heart disease, hypertension, diabetes, AIDS and asthma. The effort aims to reduce discomfort within Black communities about seeking health care, either due to concerns about racism or a historical distrust of science and government.
The initiative has so far been responsible for over 30,000 vaccinations in the first three months in 50 churches in New York; Newark, New Jersey; Detroit; Washington, D.C.; and Atlanta.
The federal funding will expand the group’s effort to 100 churches, including in rural areas, in 13 states and the District of Columbia, and will help establish an infrastructure for the health navigators to start screenings. Quest Diagnostics and its foundation has already provided funding and testing help.
Choose Healthy Life expects to be involved for at least five years, after which organizers hope control and funding will be handled locally, possibly by health departments or in alignment with federally supported health centers, Fraser-Howze said.
The initiative is also planning to host seminars in churches on common health issues. Some churches already have health clinics and they hope that encourages other churches to follow suit, said Fraser-Howze, who led the National Black Leadership Commission on AIDS for 21 years.
FILE – In this file photo taken June 6, 2021, first lady Jill Biden, center left, Dr. Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases, Choose Healthy Life public health navigator Linda Thompson and Choose Healthy Life Founder Debra Fraser-Howze, far right, speak to a person as they visit a vaccine clinic at the Abyssinian Baptist Church in the Harlem neighborhood of New York. The church is part of Choose Healthy Life, a national initiative involving Black clergy, United Way of New York City and others, that has just been awarded a $9.9 million U.S. Department of Health and Human Services grant to expand vaccinations and provide screening and other health services in churches. (AP Photo/Craig Ruttle, File)
“The Black church is going to have to be that link between faith and science,” she said.
In Milwaukee, nearly 43% of all coronavirus-related deaths have been in the Black community, according to the Milwaukee Health Department. Census data indicates Blacks make up about 39% of the city’s population. An initiative involving Pastors United, Milwaukee Inner City Congregations Allied for Hope and Souls to the Polls has provided vaccinations in at least 80 churches there already.
Milwaukee is one of the most segregated cities in the country, according to the studies by the Brookings Institution. Ericka Sinclair, CEO of Health Connections, Inc., which administers vaccinations, says that’s why putting vaccination centers in churches and other trusted locations is so important.
“Access to services is not the same for everyone. It’s just not. And it is just another reason why when we talk about health equity, we have … to do a course correction,” she said.
She’s also working to get more community health workers funded through insurance companies, including Medicaid.
The church vaccination effort involved Milwaukee Inner City Congregations Allied for Hope, which is faith organization working on social issues. Executive Director and Lead Organizer Lisa Jones says the effect of COVID-19 on the Black community has reinforced the need to address race-related disparities in health care. The group has hired another organizer to address disparities in hospital services in the inner city and housing, and lead contamination.
At a recent vaccination clinic in Milwaukee at St. Matthew, a Christian Methodist Episcopal church, Melanie Paige overcame her fears to get vaccinated. Paige, who has lupus and rheumatoid arthritis, said the church clinic helped motivate her, along with encouragement from her son.
“I was more comfortable because I belong to the church and I know I’ve been here all my life. So that made it easier.”
___
Associated Press religion coverage receives support from the Lilly Endowment through The Conversation U.S. The AP is solely responsible for this content.
In the middle of lively conversation over dinner with a friend recently, he paused, closed his eyes, and took a deep breath while placing his hand over his chest. The pain was evident on his face. When I asked what was wrong, he shared that he had been experiencing chest pains and fatigue with regular occurrence.
“Have you been to the doctor?” I asked.
“Nah. It’s probably anxiety. I’ve been stressed at work lately.”
We talked honestly about the severity of his symptoms and when they started. And because we’re cool, I asked about the results from his latest physical examination. Turns out, not only had he not seen a doctor about his recent episodes, he had not had a regular check-up in three years. I urged him to go to the doctor as soon as possible in the event that his symptoms were evidence of a significant illness.
Health is wealth.
African Proverb
If health is wealth, and it is, then many African Americans are guilty of not knowing the balance in our accounts. Meaning, annual check-ups and preventative care are not what we do. For my friend, it was a perceived lack of time that moved annual doctor’s visits to the bottom of his list of priorities. I can identify with him. While I do not skip my annual visits to my primary care physician and gynecologist, often when I am sick, I ignore the symptoms. My husband has to gently encourage me to call the doctor. Between keeping up home, shuttling our girls to their activities, ministry, and work, who has time to sit in a waiting room for hours?
For others, lack of insurance coverage, fear of disease, and historic exploitation of black bodies in medical science that fostered a distrust of doctors keeps them from scheduling preventative exams and following up on symptoms. The reality is that preventative care costs less than treating a preventable disease and browsing Dr. Google can invoke more fear that having concrete information and making informed decisions about your health. There is also the systemic racism, trauma and devaluing of our bodies that African Americans have and continue to face — experiences that have caused us to normalize pain to the point that we ignore the signs when our bodies are suffering. I am reminded of the woman recorded in Luke 13:10-17 who was bent over for eighteen years. The Bible does not tell us that at any point she sought healing. She went about her business living in chronic pain until Jesus saw her and healed her.
We are living in grind culture, where many of us skimp on sleep and spend countless hours scrolling on devices while eating conveniently packaged foods packed with sodium, fat, and sugar. And although African Americans are living longer in general, reports show that younger African Americans (18-49) are afflicted with and dying of treatable diseases like heart disease, stroke, and complications from diabetes at an alarming rate, according to the CDC. In fact, younger African Americans are living with diseases that commonly affected older adults. The stressors from unemployment, underemployment, poverty, and lack of access to healthcare negatively impacts their health. We are living longer, but we are getting sick earlier.
I shall not die, but I shall live, and recount the deeds of the Lord.
Psalm 118:17 (NRSV)
What are we to do? The first thing is to make a decision to live. Part of that decision is to make annual physical examinations a priority. As the proverb goes, “An ounce of prevention is worth a pound of cure.” I schedule all of my appointments—annual physical, gynecological exam, mammogram, and eye examination around my birthday. Doing so helps me to remember my appointments and also helps me to recognize the blessed gift of life that God has given me to steward. The other part of that decision to live is to listen to our bodies and to follow up with a doctor if even the slightest thing is off, with the recognition that we are worthy of care and that we do not have to live with chronic pain and disease.
Because our health is so valuable and important, I would suggest finding doctors that you feel comfortable with, that you can trust, and that are sensitive to your particular needs. Word of mouth from family, friends, and coworkers is the best way to find a good doctor. Developing a relationship with a doctor will also allow them to know your baseline levels, recognize patterns in your health, and know immediately when something needs additional attention.
The bottom line is that we have to see our doctors as if our lives depend on it…because they do. Whether you need to cram in a visit to the health center in-between college classes or you are scheduling your very first mammogram, here’s a list of the exams you need by decade, courtesy of Tri-City Medical Center:
For informational purposes only. The information in this article is not intended to replace a one-on-one relationship with a qualified health care professional and is not intended as medical advice.
Rev. Donna Olivia Owusu-Ansah is a preacher, chaplain, teacher, artist, writer, thinker, and dreamer who loves to study the Word of God, encourage others, and worship God. Rev. Owusu-Ansah holds a BS in Studio Art from New York University, an MFA in Photography from Howard University, and a Master of Divinity, Pastoral Theology, from Drew University. You can check out her website at https://www.reverendmotherrunner.com.
Actor Chadwick Boseman at the GQ Men of the Year party at the Chateau Marmont in Los Angeles, Dec. 3, 2015. Jordan Strauss/Invision/AP
The tragic death of Chadwick Boseman at age 43 following a four-year battle against colorectal cancer underscores two important public health concerns.
First, the incidence of colorectal cancer has risen dramatically among adults under age 50 in the U.S. and in many countries around the world. Second, African Americans have a much greater likelihood of being diagnosed and dying from the disease at any age. Both issues are important to the public health community and efforts are ongoing to address them.
Colorectal cancer remains a major source of cancer incidence and death in the U.S. The American Cancer Society estimates that in 2020, about 147,950 people will be diagnosed with colorectal cancer and 53,200 will die from the disease, making it the fourth most prevalent form of cancer and the second leading cause of cancer mortality.
In 2017, Dr. Rebecca Siegel and colleagues published detailed and compelling statistical data clearly bringing the issue into sharp focus, stimulating greater coverage in the media.
Analysis of trends in colorectal cancer incidence and mortality have clearly shown a decline in the general U.S. population overall during the past few decades. Unfortunately, this has not been the case for young adults.
For example, incidence has decreased by an average of 4% per year between 2007 and 2016 in those over 65 years of age, in contrast to an increase of 1.4% per year during the same period in those under 50. The observed decrease in older adults is likely due to preventive screening, which is recommended and advocated for people over 50 and has been undertaken by a larger fraction of the population.
Similarly, colorectal cancer mortality has declined by 3% per year between 2008 and 2017 in those over 65, while it has increased by 1.3% per year in those under 50.
I have met a number of young people, including several in their 20s and 30s, who had been diagnosed with colorectal cancer and were in the midst of fighting it. I have also met parents who lost young adult children to the disease, and were still trying to understand how this could have happened.
I have been struck by the intensity and complexity of emotions displayed by these people, including anger, resentment, embarrassment, hopelessness, fear and resolve. While a cancer diagnosis at any age is scary and disorienting, it extracts a particularly powerful psychological and social toll on young adults.
What is causing the increase in young adults? We do not know for certain. Several studies have indicated that the disease in young people is different with regard to the specific location of the tumor within the colon or rectum.
Also, the pathology, genetics and response to treatment differ. Lifestyle trends, such as overweight and obesity, lack of physical activity and changing diets, have been suggested to play roles. Studies have indicated that obesity is associated with increased risk of early-onset colorectal cancer in women.
While these trends may contribute, they are not fully explanatory. Physicians have told me anecdotally that many of their younger patients are thin, fit, physically active and in general good health, suggesting that something else must be going on.
What could that something else be? One intriguing possibility may lie in the billions of microbes, collectively termed the microbiota, that live on and within our bodies. Preliminary findings reported at the 2020 Gastrointestinal Symposium recently indicated that there may be differences between the microbiota within tumors from younger versus older colorectal cancer patients.
The death of Boseman has also underscored the long-standing racial disparity for colorectal cancer. African Americans suffer from high incidences and mortalities, regardless of age. Incidence in African Americans was 18% higher than in whites during 2012-2016, while mortality was 38% higher during the same period. For reasons we do not yet know, incidence in younger African Americans has been relatively stable in contrast to that in younger whites.
Increased incidence and death from colorectal cancer in African Americans is likely a consequence of lower rates of screening, as well as environmental, socioeconomic and lifestyle factors. Reduction of the disparities may depend upon addressing these factors.
Screening can prevent colorectal cancer
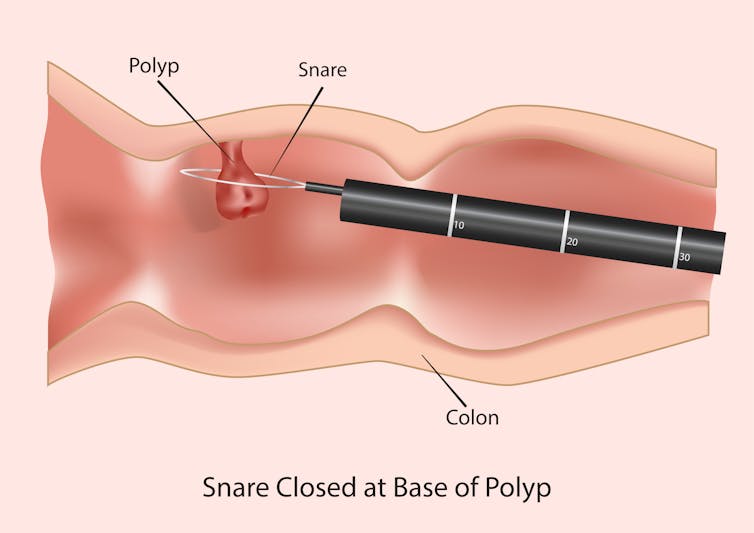
Precancerous growths called polyps can be easily removed during a colonoscopy. Sezer33/Shutterstock.com
Screening for colorectal cancer not only detects the disease but is also highly effective in preventing it. Screening can readily identify precancerous growths called polyps, as well as early-stage cancers. These often can be removed before they progress to life-threatening stages.
In addition, research is underway to find new methods for colorectal cancer screening based upon analysis of easily obtained body fluids such as blood and urine.
Based upon the knowledge that about 90% of colorectal cancer cases occurs in those 50 and over, the U.S. Preventive Services Task Force currently recommends that screening should begin at age 50 for those who have no predisposing symptoms. This population is experiencing the decrease in colorectal cancer incidence and death that is currently being observed overall.
But screening is not typically recommended for those under 50, and most health insurers do not pay for screening in this group.
This lack of screening, combined with a general lack of awareness about colorectal cancer and its symptoms among young people can result in late diagnoses. Later diagnoses can often result in more advanced stages of the disease, when it is harder to treat and significantly more lethal.
There is also a need to increase screening in the African American community. At present, recommendations vary. In contrast to the U.S. Preventive Services Task Force and the CDC, the U.S. Multi-Society Task Force recommends that screening in African Americans should begin at age 45 rather than 50. I hope these influential organizations will reach a consensus on this issue.
Sorting out the causes of age and race disparities in colorectal cancer incidences and mortalities, and understanding the nature of the disease more thoroughly, will take time.
As Boseman’s untimely death reminds us, colorectal cancer is a difficult and emotional disease for all people at any age. Awareness of signs and symptoms, along with engagement in screening as appropriate, will lead to the eventual eradication of the disease as a major form of cancer.